
1. Switching to Oral Therapy
1.1. factors to consider
1.1.1. fever
1.1.2. respiratory fxn (O2 sat>90, RR<24)
1.1.3. WBC count
1.1.4. GI (able to tolerate PO)
1.1.5. mental status at baseline
1.2. delay when
1.2.1. more than one factor
1.2.2. initial therapy failure/switched
1.2.3. other infxn (meningitis/endocarditis)
1.2.4. documented Pseudomonas/Stap/Other bug
1.3. No need to observe overnight in hospital when switching!
2. FU CXR
2.1. Not necessary, and NOT linked to clinical status!
2.2. In smoker age > 40, can help R/O malignancy after 7-12 wks
2.3. If pt improving, no routine CXR needed
3. Pseudomonas
3.1. Tx
3.1.1. Antipneumococcal Antipseudococcal beta-lactam
3.1.1.1. + either
3.1.1.1.1. Anti-Pseudomonal Fluoroquinolone
3.1.1.1.2. Aminoglycoside
3.1.2. Beta-Lactam Allergy
3.1.2.1. Aztreonam
3.1.2.1.1. +
3.2. Risk Factors
3.2.1. Bronchiectasis/COPD/Chronic Lung disease
3.2.1.1. Requiring frequent antibiotics
3.2.1.2. Requiring frequent steroids
4. CA-MRSA
4.1. Risk Factors
4.1.1. Prior Abx
4.1.2. Recent flu-like illness
4.1.3. IV Drug use
4.1.4. Contact sports
4.1.5. Men who have sex with men
4.1.6. Prisoners
4.2. Tx
4.2.1. Anti-Staph Antibiotic
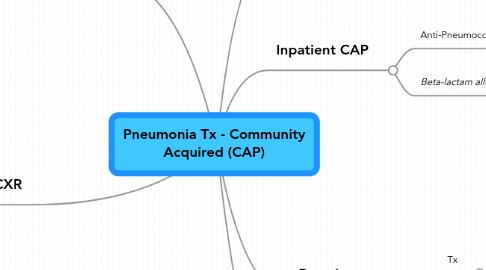
5. Inpatient CAP
5.1. Anti-Pneumococcal beta-lactam
5.1.1. + either
5.1.1.1. Azithromycin
5.1.1.2. Respiratory fluoroquinolone
5.2. Beta-lactam allergy
5.2.1. Aztreonam
5.2.1.1. +
5.2.1.1.1. Respiratory fluoroquinolone
6. Outpatient
6.1. Tx
6.1.1. Previously Healthy
6.1.1.1. General Respiratory Antibiotic (macrolide/doxy)
6.1.2. Comorbidities or regional DRSP
6.1.2.1. either
6.1.2.1.1. Respiratory Fluoroquinolone
6.1.2.1.2. Beta-Lactam + Macrolide