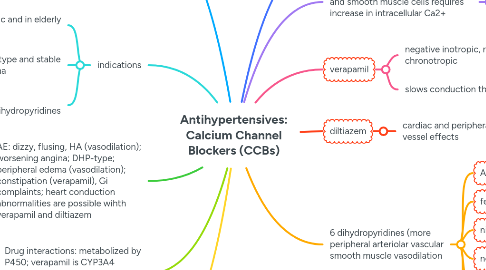
3. AE: dizzy, flusing, HA (vasodilation); worsening angina; DHP-type; peripheral edema (vasodilation); constipation (verapamil), Gi complaints; heart conduction abnormalities are possible wihth verapamil and diltiazem
4. Drug interactions: metabolized by P450; verapamil is CYP3A4 inhibitor: verapamil may increase toxicity of digoxin, theophylline, and other drugs
5. CI: use cuation when combine CCBs with beta blockers; severe congestive heart failure and high degree heart blocks for non DHP; diltiazem and verapamil: severe hypotention, sick sinus syndrome, high degree AV block
6. First line HTN drugs
7. Background: contraction of cardiac and smooth muscle cells requires increase in intracellular Ca2+
7.1. Calcium->binds to calmodulin->acivates actin and myosin->muscle contration