

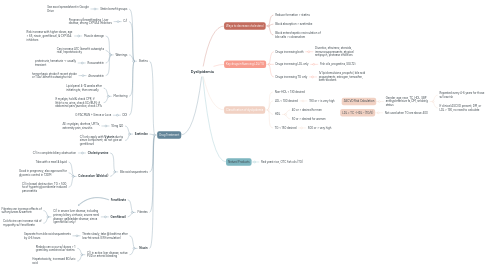
1. Ways to decrease cholesterol
1.1. Reduce formation > statins
1.2. Block absorption > ezetimibe
1.3. Block enterohepatic recirculation of bile salts > colesevelam
2. Key drugs influencing LDL/TG
2.1. Drugs increasing both
2.1.1. Diuretics, efavirenz, steroids, immunosuppressants, atypical antipsych, protease inhibitors
2.2. Drugs increasing LDL only
2.2.1. Fish oils, progestins, SGLT2i
2.3. Drugs increasing TG only
2.3.1. IV lipid emulsions, propofol, bile acid sequestrants, estrogen, tamoxifen, beta-blockers
3. Classification of dyslipidemia
3.1. Non-HDL < 130 desired
3.2. LDL < 100 desired
3.2.1. 190 or > is very high
3.3. HDL
3.3.1. 40 or > desired for men
3.3.2. 50 or > desired for women
3.4. TG < 150 desired
3.4.1. 500 or > very high
4. LDL = TC - HDL - (TG/5)
4.1. Not used when TG are above 400
5. ASCVD Risk Calculation
5.1. Gender, age, race, TC, HDL, SBP, antihypertensive tx, DM, smoking status
5.1.1. Repeated every 4-6 years for those w/ low risk
5.1.2. If clinical ASCVD present, DM, or LDL > 190, no need to calculate
6. Natural Products
6.1. Red yeast rice, OTC fish oils (TG)
7. Drug Treatment
7.1. Statins
7.1.1. Statin benefit groups
7.1.1.1. See excel spreadsheet in Google Drive
7.1.2. C/I
7.1.2.1. Pregnancy/breastfeeding, Liver disease, strong CYP3A4 inhibitors
7.1.3. Warnings
7.1.3.1. Muscle damage
7.1.3.1.1. Risk increase with higher doses, age > 65, niacin, gemfibrozil, & CYP3A4 inhibitors
7.1.3.2. Can increase A1C (benefit outweighs risk), hepatotoxicity
7.1.3.3. Rosuvastatin
7.1.3.3.1. proteinuria, hematuria -> usually transient
7.1.3.4. Atorvastatin
7.1.3.4.1. hemorrhagic stroke if recent stroke or TIAs (benefit outweighs risk)
7.1.4. Monitoring
7.1.4.1. Lipid panel 4-12 weeks after initiating tx, then annually
7.1.4.2. If myalgia, hold & check CPK; if little to no urine, check SCr/BUN; if abdominal pain/jaundice, check LFTs
7.1.5. DDI
7.1.5.1. G PACMAN + Simva or Lova
7.2. **Ezetimibe**
7.2.1. 10mg QD
7.2.1.1. AE: myalgias, diarrhea, URTIs, extremity pain, sinusitis
7.2.2. C/I only apply with **Vytorin** due to simva component; do not give w/ gemfibrozil
7.3. Bile acid sequestrants
7.3.1. **Cholestyramine**
7.3.1.1. C/I in complete biliary obstruction
7.3.2. **Colesevelam (Welchol)**
7.3.2.1. Take with a meal & liquid
7.3.2.2. Good in pregnancy; also approved for glycemic control in T2DM
7.3.2.3. C/I in bowel obstruction, TG > 500, hx of hypertriglyceridemia-induced pancreatitis
7.4. Fibrates
7.4.1. **Fenofibrate**
7.4.2. **Gemfibrozil**
7.4.2.1. C/I in severe liver disease, including primary biliary cirrhosis; severe renal disease; gallbladder disease; simva (gemfibrozil only)
7.4.2.1.1. Fibrates can increase effects of sulfonylureas & warfarin
7.4.2.1.2. Colchicine can increase risk of myopathy w/ fenofibrate
7.5. **Niacin**
7.5.1. Titrate slowly; take @ bedtime after low-fat snack (ER formulation)
7.5.1.1. Separate from bile acid sequestrants by 4-6 hours
7.5.2. C/I in active liver disease, active PUD or arterial bleeding
7.5.2.1. Rhabdo can occur w/ doses > 1 gram/day combined w/ statins
7.5.2.2. Hepatotoxicity, increased BG/uric acid