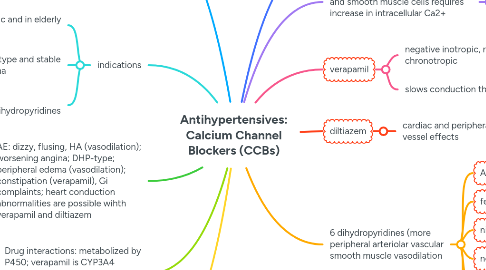
Antihypertensives: Calcium Channel Blockers (CCBs)
作者:Anneke Klomp
1. MOA: CCBs inhibit influx fo Ca++
1.1. causes peripheral artery dilation and coronary arteries dilate
1.2. also slows conduction through AV node, reduces contractility of myocardial muscle, slows rate of sinus node
1.3. Ca is needed to sustain AP and cause muscle contraction
2. indications
2.1. HTN (esp systolic and in elderly pts)
2.2. angina: variant type and stable exertional angina
2.3. SVT (supraventricular tachyarrhythmias): non-dihydropyridines
3. AE: dizzy, flusing, HA (vasodilation); worsening angina; DHP-type; peripheral edema (vasodilation); constipation (verapamil), Gi complaints; heart conduction abnormalities are possible wihth verapamil and diltiazem
4. Drug interactions: metabolized by P450; verapamil is CYP3A4 inhibitor: verapamil may increase toxicity of digoxin, theophylline, and other drugs
5. CI: use cuation when combine CCBs with beta blockers; severe congestive heart failure and high degree heart blocks for non DHP; diltiazem and verapamil: severe hypotention, sick sinus syndrome, high degree AV block
6. First line HTN drugs
7. Background: contraction of cardiac and smooth muscle cells requires increase in intracellular Ca2+
7.1. Calcium->binds to calmodulin->acivates actin and myosin->muscle contration
8. verapamil
8.1. negative inotropic, negative chronotropic
8.2. slows conduction through AV node
9. diltiazem
9.1. cardiac and peripheral blood vessel effects
10. 6 dihydropyridines (more peripheral arteriolar vascular smooth muscle vasodilation
10.1. Amlodipine
10.2. felodipine
10.3. nicardipine
10.4. nefedipine
10.5. isradipine
10.6. nisoldipine

