Life Long Learning Project: Breast Cancer

Plan your life and the next important steps and goals to proceed with a happy life

1. Epidemiology
1.1. Epidemiology 1. Most common cancer in N. American females 2. Second most common cause of cancer-related deaths in women 3. Increasing incidence with age (median age is 64) 4. Male breast cancer comprises <1% of all cases (Female to male ratio 150:1) 5. Genetic factors: first degree relative with breast cancer increases risk, hereditary breast cancer syndromes (eg., BRCA 1 and 2, Li-Fraumeni syndrome, Lynch syndrome) 6. BRCA 1 increases risk for breast, colon, ovarian and prostate cancers 7. BRCA 2 increases risk for breast cancer (including male breast cancer) and pancreatic cancers (lower risk for ovarian cancer compared with BRCA 1) 8. The vast majority (90%) of cases of breast cancer are “sporadic” 9. Endocrine risks: prolonged endogenous estrogen from early menarche, late parity, nulliparity or late menopause increases risk. Small increased risk with post-menopausal hormone replacement therapy (greatest with combined estrogen and progesterone), but not with oral contraceptives 10. High fat diet, obesity, alcohol consumption, and possibly smoking are other risk factors (note: women who drink alcohol and take folic acid can have a modified reduced risk compared, but folic acid shows no improvement in women who abstain from alcohol.) 11. Ionizing radiation increases risk (in developing years) 12. History of atypical hyperplasia increases risk 4-5X 13. LCIS/DCIS increases risk 8-10X
2. Pathophysiology
2.1. 1. Non-invasive include ductal carcinoma in situ (DCIS) which is a pre-cursor to invasive cancer; frequently accompanies invasive cancer; lobular carcinoma in situ (LCIS) is not cancer but indicates a high risk and carries an equal risk in either breast
2.2. 2. Invasive forms include adenocarcinomas that are derived from a breast gland duct (infiltrating ductal carcinoma) or milk producing cell (infiltrating lobular carcinoma); 80% are infiltrating ductal carcinoma
2.3. 3. Other less common invasive types include medullary carcinoma (5%) which grow larger and are well circumscribed; they carry a better prognosis
2.4. 4. Most aggressive and lethal form is inflammatory breast cancer; manifests as skin redness and warmth, induration of the underlying breast; cells infiltrate and obstruct subdermal lymphatics
2.5. Categories
2.5.1. Infiltrating ductal - 76 percent ●Invasive lobular - 8 percent ●Ductal/lobular - 7 percent ●Mucinous (colloid) - 2.4 percent ●Tubular - 1.5 percent ●Medullary - 1.2 percent ●Papillary - 1 percent
2.5.2. Other subtypes, including metaplastic breast cancer and invasive micropapillary breast cancer, all account for fewer than 5 percent of cases
3. Symptoms
3.1. Fatigue
3.2. Unintentional weight loss
3.3. Pain in the affected breast (unilateral)
3.4. Metastatic symptoms: cough, hemoptysis, dyspnea, bone pain, neurologic symptoms, weight loss
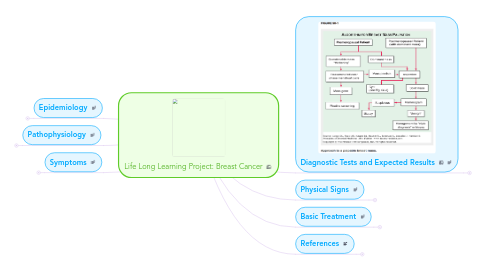
4. Diagnostic Tests and Expected Results
4.1. Screening 1. Monthly breast self-exam (not proven to improve on mortality) 2. Yearly MD exam 3. Annual mammograms over the age 50 up to age 70 4. Mammograms prior to age 50 and over age 70 less proven 5. High risk women should have mammograms or MRI at an earlier age 6. MRI may be better in high risk women, including those with BRCA mutations; MRI is more sensitive than Mammography but MRI also has a high false positive rate
4.2. Work-up
4.2.1. 1. Mammogram of both breasts
4.2.2. 2. A “negative” mammogram in the face of a suspicious palpable mass should be evaluated further.
4.2.3. 3. FNA or core biopsy or excisional biopsy for diagnosis pursued with an ultrasound and/or tissue diagnosis
4.2.4. 4. All tumors should be evlauated for hormone status (ER, PR) and the presence of Her-2-neu overexpression; these have both prognostic significance and clinical implications