

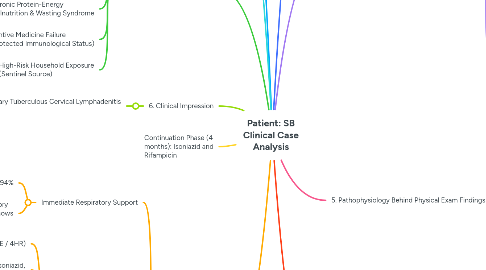
1. 1. Patient Profile
1.1. 6-year-old female from Basilan
1.2. CC: FEVER
2. Pediatric age (6 years) with immature cell-mediated immunity
3. 2. Risk Factors
3.1. Household Exposure
3.1.1. Grandmother with chronic cough and breathing difficulty
3.1.2. Crowded household with 10 siblings
3.2. Immunological
3.2.1. No BCG vaccination at birth
3.3. Nutritional
3.3.1. Weight 15 kg (significantly low for age)
3.3.2. Loss of appetite
3.3.3. Chronic recurrent fevers
3.4. Geographic and Socioeconomic
3.4.1. Resides in Basilan City, high TB prevalence area
3.4.2. Low socioeconomic status (self-employed family)
3.5. Host Biology
4. 3. Signs and Symptoms with Pathophysiology
4.1. Respiratory
4.1.1. Extreme tachypnea (RR 68 bpm)
4.1.2. Alar flaring and intercostal/supraclavicular retractions
4.1.3. Right-sided dullness on percussion with increased tactile and vocal fremitus
4.1.4. Crackles
4.2. Lymphatic and Integumentary
4.2.1. Matted bilateral cervical lymphadenopathy
4.2.2. Right supraclavicular scrofuloderma (4x4 cm)
4.3. Constitutional
4.3.1. High-grade fever (39°C)
4.3.2. Weight loss and wasting
4.3.3. Tachycardia
5. 4. Clinical Problems Identified
5.1. Impending Respiratory Failure secondary to Severe Lobar Consolidation
5.1.1. Impending Respiratory Failure due to severe V/Q mismatch and reduced lung compliance
5.2. Disseminated Tuberculosis (Pulmonary and Extrapulmonary)
5.3. Acute Systemic Inflammatory Response Syndrome (SIRS)
5.4. Chronic Protein-Energy Malnutrition & Wasting Syndrome
5.5. Preventive Medicine Failure (Unprotected Immunological Status)
5.6. High-Risk Household Exposure (Sentinel Source)
6. 5. Pathophysiology Behind Physical Exam Findings
6.1. Dullness with increased fremitus
6.2. Matted cervical lymph nodes
6.3. Scrofuloderma
6.4. Alar flaring and retractions
6.5. Crackles
6.6. Tachycardia
7. 6. Clinical Impression
7.1. Disseminated TB with Primary Progressive Tuberculosis with miliary pattern and Extrapulmonary Tuberculous Cervical Lymphadenitis (Scrofula) with Scrofuloderma
8. Continuation Phase (4 months): Isoniazid and Rifampicin
9. 7. Paraclinical Diagnostics
9.1. Bacteriological
9.1.1. Gastric Aspirate (3 mornings) for Xpert MTB/RIF and AFB Culture
9.1.2. Needle biopsy of scrofuloderma for Xpert and Histopathology
9.2. Radiology
9.2.1. Chest X-ray PA and Lateral
9.3. Immunological and Adjunctive
9.3.1. Tuberculin Skin Test (TST)
9.3.2. Complete Blood Count (CBC)
9.4. Physiological
9.4.1. Pulse oximetry and Arterial Blood Gas (ABG)
10. 8. Management
10.1. Immediate Respiratory Support
10.1.1. Supplemental oxygen to maintain SpO2 > 94%
10.1.2. Evaluate for ICU if respiratory distress worsens or ABG shows severe hypoxia
10.2. Pharmacological Treatment
10.2.1. Category I Pediatric Regimen (2HRZE / 4HR)
10.2.2. Intensive Phase (2 months): Isoniazid, Rifampicin, Pyrazinamide, Ethambutol
10.2.3. Adjuvant corticosteroids: Prednisone 2 mg/kg/day for 4-6 weeks to reduce inflammation
10.3. Supportive Care
10.3.1. Nutritional support with high-protein, calorie-dense diet
10.3.2. Pyridoxine supplementation to prevent isoniazid neuropathy
10.3.3. Active Drug Safety Monitoring (hepatotoxicity, optic neuritis)
10.4. Public Health Measures
10.4.1. Urgent contact investigation for 10 siblings and household members
10.4.2. TB Preventive Treatment (TPT) for exposed siblings <5 years old
10.5. Clinical Monitoring
10.5.1. Monitor respiratory rate normalization within 48-72 hours
10.5.2. Monitor fever defervescence within 7-14 days
10.5.3. Monitor weight gain monthly
10.5.4. Monitor healing of scrofuloderma; consider surgical drainage if needed