

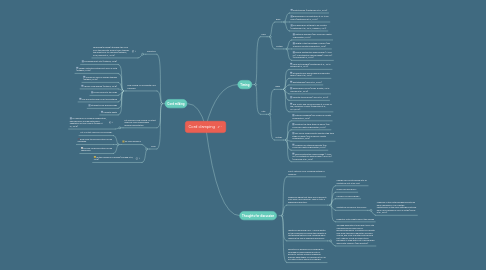
1. Cord milking
1.1. Definition
1.1.1. squeezing/pushing/"stripped" the cord from the placenta several times towards the infant prior to clamping (Katheria, 2018, Basile et al., 2019)
1.2. cord milking vs. immediate cord clamping
1.2.1. increased heart rate (Katheria, 2018)
1.2.2. oxygen saturation within first 5min of birth (Katheria, 2018)
1.2.3. number of days on oxygen therapy (Katheria, 2018)
1.2.4. chronic lung disease (Katheria, 2018)
1.2.5. blood volume to the lungs
1.2.6. may promote earlier onset of breathing
1.2.7. intraventricular haemorrhage
1.2.8. neonatal death
1.3. cut umbilical cord milking vs. intact umbilical cord milking when needing resuscitation
1.3.1. no difference in cerebral oxygenation, hemodynamic and hematological adaptation of term infants (Orpak et al., 2019)
1.4. Issue
1.4.1. no clear guidance
1.4.1.1. cut or intact umbilical cord milking?
1.4.1.2. how many times should the cord be squeezed
1.4.1.3. for how long should the cord be squeezed?
1.4.2. further research is needed (Kilicdag et al, 2016)
2. Timing
2.1. Early
2.1.1. Baby
2.1.1.1. Phototherapy (Palethorpe et al., 2010)
2.1.1.2. haemoglobin concentration at 24 to 48 hours (Palethorpe et al., 2010)
2.1.1.3. iron deficiency at three to six months (Palethorpe et al., 2010, Chaparro, 2011)
2.1.2. Mother
2.1.2.1. maternal bleeding (Pan American Health Organization, 2013)
2.1.2.2. length of the third stage of labour (Pan American Health Organization, 2013)
2.1.2.3. severe postpartum haemorrhage (>1000 mL) or postpartum haemorrhage (>500 mL) (McDonald et al., 2013)
2.2. Late
2.2.1. Baby
2.2.1.1. mean birth weight (Palethorpe et al., 2010; Katheria et al., 2017)
2.2.1.2. intraventricular hemorrhage and neonatal sepsis (Jelin et al., 2014)
2.2.1.3. phototherapy (Qian et al., 2020)
2.2.1.4. haemoglobin levels (Duley & Batey, 2013; Nouraie et al., 2019)
2.2.1.5. neonatal transfusions (Jelin et al., 2014)
2.2.1.6. fine-motor and social domains at 4 years of age, especially in boys (Andersson et al., 2014,2015).
2.2.2. Mother
2.2.2.1. maternal bleeding (Pan American Health Organization, 2013)
2.2.2.2. length of the third stage of labour (Pan American Health Organization, 2013)
2.2.2.3. less blood-filled placenta shortens the third stage of labour (Pan American Health Organization, 2013)
2.2.2.4. incidence of retained placenta (Pan American Health Organization, 2013)
2.2.2.5. severe postpartum haemorrhage (>1000 mL) or postpartum haemorrhage (>500 mL) (McDonald et al., 2013)
3. Thoughts for discussion
3.1. Call it "optimal cord" clamping instead of "delayed"
3.2. Guidelines agree that there are no benefits from early cord clamping - why is it still a widespread practice?
3.2.1. change can be introduced into an obstetrical unit at no cost
3.2.2. reasons of efficiency?
3.2.3. concern for hemorrhage?
3.2.4. obstetrical led care as the cause?
3.2.4.1. Midwives in the United Kingdom practiced early clamping in 41% of births; obstetricians in the same settings practiced early cord clamping in 74% of births (Farrar et al., 2010)
3.2.5. pedeatric units might support the change
3.3. Length of remaining cord - could a length of the remaining cord allow the benefits of late/delayed/optimal cord clamping while reducing the risk of hyperbilirubinaemia?
3.3.1. Too high haematocrit may result from late clamping and increase risk for hyperbilirubinaemia. Increased cord length may allow the bayby regulation of blood volume, esp. level of erythrocytes during first 24hours. Cords are found to be bloodless or filled with a lot of blood when dryed after 48hours (own practice)