

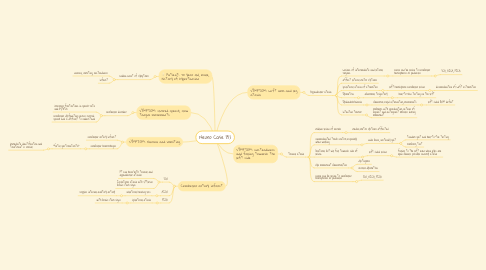
1. Patient: 70 year old, male, history of hypertension
1.1. sudden onset of symptoms
1.1.1. nausea, vomiting, unsteadiness
1.1.2. infarct
2. SYMPTOM: slurred speech, slow tongue movements
2.1. cerebellar disorder
2.1.1. irregular fluctuations in speech rate and rythtm
2.1.2. cerebellar dysfunction causes slurred speech and is difficult to understand
3. SYMPTOM: Nausea and vomiting
3.1. cerebellar artery infarct
3.2. cerebellar hemorrhages
3.2.1. "fatal gastroenteritis"
3.2.1.1. immediate identification and treatment is crucial
4. Cerebellar artery infarct
4.1. SCA
4.1.1. Pt can have both truncal and appendicular ataxias
4.1.2. Ipsilateral ataxia with little/no brain stem signs
4.2. AICA
4.2.1. unilateral hearing loss
4.2.1.1. supplies internal auditory artery
4.3. PICA
4.3.1. ipsilateral ataxia
4.3.1.1. with brain stem signs
5. SYMPTOM: Left arm and leg ataxia
5.1. Appendicular ataxia
5.1.1. Lesions of intermediate and lateral regions
5.1.1.1. cause can be lesion to cerebellar hemispheres or peduncles
5.1.1.1.1. SCA, AICA, PICA
5.1.2. affect lateral motor systems
5.1.3. ipsilateral ataxia of etremities
5.1.3.1. left hemisphere cerebellar lesion
5.1.3.1.1. discoordination of Left extremities
5.1.4. Dysmetria
5.1.4.1. abnormal trajectory
5.1.4.1.1. heel-to-shin testing on the left
5.1.5. Dysdiadochokinesia
5.1.5.1. abnormal rapid alternating movements
5.1.5.1.1. left sided RAM deficit
5.1.6. intention tremor
5.1.6.1. problems with coordinating actions of agonist and antagonist muscles during movement
6. SYMPTOM: Unsteadiness and falling towards the left side
6.1. Truncal ataxia
6.1.1. midline lesion of vermis
6.1.1.1. medial motor systems affected
6.1.2. uncoordinated trunk control especially when walking
6.1.2.1. wide base, unsteady gait
6.1.2.1.1. tandem gait and heel-to-toe testing
6.1.2.1.2. romberg test
6.1.3. bilateral but will fall towards side of lesion
6.1.3.1. left sided lesion
6.1.3.1.1. falling to the left even when eyes are open cancels possible sensory ataxia
6.1.4. eye movement abnormalities
6.1.4.1. nystagmus
6.1.4.2. occular dysmetria
6.1.5. cause can be lesion to cerebellar hemispheres or peduncles
6.1.5.1. SCA, AICA, PICA