

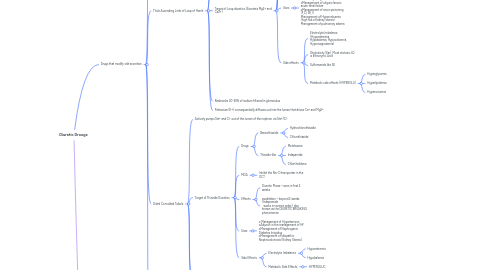
1. Drugs that modify salt excretion
1.1. Proximal Convoluted Tubule
1.1.1. Responsible for 60-70% of Na Reabsorption
1.1.2. The part of the nephron where NaHCO3 reabsorption ONLY occurs
1.1.3. NaHCO3 is poorly absorbed in lumen, it’s converted by carbonic acid into CO2 which is permeable in the lumen
1.1.4. Drugs that exert their action in the PCT
1.1.4.1. oCarbonic anhydrase inhibitors
1.1.4.1.1. “-zolamides”
1.1.4.1.2. Effects
1.1.4.1.3. Uses
1.1.4.1.4. Side Effects
1.1.4.1.5. Con't
1.1.4.2. oMethylxanthines
1.1.4.2.1. Caffeine
1.1.4.3. oOsmotic Diuretics
1.1.4.3.1. Mannitol
1.1.4.4. oAcidifying salts
1.1.4.4.1. NH4Cl
1.2. Thick Ascending Limb of Loop of Henle
1.2.1. Pumps Na+, K+, and Cl- out of lumen into interstitium of kidney by Na+/K+/2Cl transporter
1.2.2. Major site of Ca+ and Mg2+ Reabsorption
1.2.3. Target of Loop diuretics (Excretes Mg2+ and Ca2+)
1.2.3.1. High Ceiling diuretics (can be used at low GFR)
1.2.3.2. Examples
1.2.3.2.1. Sulfonamide-like: Furosemide and Bumetanide
1.2.3.2.2. Sulfonylurea-like: Torsemide
1.2.3.2.3. Phenoxyacetic acid derivative: Ethacrynic acid
1.2.3.3. MOA
1.2.3.3.1. Inhibition of Na/K/2Cl cotransporter in the TAL of the loop of henle
1.2.3.4. Uses
1.2.3.4.1. oAdjunct in management of HF and Pulmonary congestion oManagement of oliguric/anuric acute renal failure oManagement of anion poisoning (F,Cl, Br, I) Management of Hypercalcemia (high risk of kidney stones) Management of pulmonary edema
1.2.3.5. Side effects
1.2.3.5.1. Electrolyte Imbalance (Hyponatremia, Hypokalemia, Hypocalcemia, Hypomagnesemia)
1.2.3.5.2. Ototoxicity (Ear), Most ototoxic LD is Ethacrynic Acid
1.2.3.5.3. Sulfonamide like SE
1.2.3.5.4. Metabolic side effects (HYPERGLU)
1.2.4. Reabsorbs 20-30% of sodium filtered in glomerulus
1.2.5. Potassium (K+) consequentially diffuses out into the lumen that drives Ca+ and Mg2+
1.3. Distal Convolted Tubule
1.3.1. Actively pumps Na+ and Cl- out of the lumen of the nephron via Na+/Cl-
1.3.2. Target of Thiazide Diuretics
1.3.2.1. Drugs
1.3.2.1.1. Benzothiazide
1.3.2.1.2. Thiazide-like
1.3.2.2. MOA
1.3.2.2.1. Inhibit the Na-Cl transporter in the DCT
1.3.2.3. Effects
1.3.2.3.1. Diuretic Phase – seen in first 2 weeks
1.3.2.3.2. asodilation – beyond 2 weeks (Indapamide works in reverse order); also known as the DIURETIC BREAKING phenomenon
1.3.2.4. Uses
1.3.2.4.1. o Management of Hypertension oAdjunct in the management of HF oManagement of Nephrogenic Diabetes Insipidus oManagement of Idiopathic Nephrocalcinosis (Kidney Stones)
1.3.2.5. Side Effects
1.3.2.5.1. Electrolyte Imbalance
1.3.2.5.2. Metabolic Side Effects
1.3.3. Responsible for 4-8% of filtered sodium reabsorption
1.3.4. Calcium is reabsorbed in this segment
1.4. Cortical Collecting Tubule
1.4.1. Final segment of the nephron is the **last tubular site of sodium reabsorption** and is **controlled by aldosterone,** a steroid hormone secreted by the adrenal cortex
1.4.2. Reabsorbs 2-5% of the total filtered sodium and accompanied by potassium and hydrogen ion loss through the ENaC (Epithelial Sodium Channels)
1.4.3. Primary site of urine acidification
1.4.4. Targeted by Potassium-sparing diuretics. (K stays in the body)
1.4.4.1. Can cause hyperkalemia
1.4.4.2. Types
1.4.4.2.1. Aldosterone Antagonists
1.4.4.2.2. Direct NaCl transport inhibitor
1.4.4.3. Uses
1.4.4.3.1. ● Prevention and treatment of hypokalemia (Both) ● Management of Hypertension secondary to aldosteronism (aldosterone antagonist) ● Management of peripheral edema in patients with chronic liver disease.
1.4.4.4. Side Effects
1.4.4.4.1. ● Hyponatremia and Hyperkalemia ●Spironoloactone – antiandrogenic effects (Male: gynecomastia, Female: infertility)
1.4.4.4.2. Triamterene: Kidney Stone Formation
2. Drugs that modify water excretion
2.1. Osmotic Diuretics
2.1.1. Mannitol, prototype osmotic diuretic, is usually given intravenously
2.1.2. Major location of action is at the PCT, Some action also occur in the Descending Loop of Henle
2.1.3. MOA
2.1.3.1. Create an osmotic gradient in the water permeable regions of the renal tubule
2.1.4. Con't
2.1.4.1. Lowers intracranial pressure in hemorrhage, lowes intraocular pressure in glaucoma
2.1.5. Side Effects
2.1.5.1. Hypovolemia and Hypernatremia
2.2. ADH Agonists
2.2.1. ADH (AKA Vasopressin)
2.2.2. Desmopressis
2.2.3. Use
2.2.3.1. Diabetes insipidus (Lack of ADH)
2.3. ADH Antagonists
2.3.1. Tolvaptan, Conivaptan, Demeclocycline
2.3.2. Tx of heart failure (most used tx is loop diuretic
2.3.3. Mainly used for SIADH ( syndrome of inappropriate ADH secretion)