

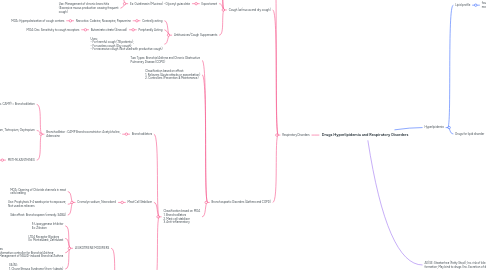
1. Hyperlipidemia
1.1. Lipid profile
1.1.1. four main quantities are measured
1.1.1.1. cholesterol, triglycerides (TAGs), LDL, and HDL
1.2. Drugs for lipid disorder
1.2.1. Statins/HMG CoA reductase Inhibitors
1.2.1.1. MOA: HMG CoA reductase Inhibitors
1.2.1.2. Decreases Cholesterol Synthesis, • Liver will utilize alternative cholesterol synthesis for bile acid synthesis • Increased hepatic LDL receptors leading to Inc. HDL and Dec. LDL
1.2.1.3. 1st line for high cholesterol
1.2.2. Fibrates/Fibric acid derivatives
1.2.2.1. MOA: Stimulates Lipase
1.2.2.2. Decreases VLDL and Serum Triglycerides
1.2.2.3. Ex: Gemfibrozil, Fenofibrate
1.2.2.3.1. Use: 1st Line of treatment for Hypertrglyceridemia
1.2.2.4. Adverse effects: - Rhabdomyolysis - Inc. Risk of Bile stone of Formation - Hepatobiliary Carcinoma
1.2.3. Nicotinic acid/Niacin
1.2.3.1. MOA: Inhibits synthesis and release VLDL and Stimulates Lipoprotein Lipase (LPL)
1.2.3.2. Niacin inhibits HDL breakdown = Inc. LPL
1.2.3.2.1. Use: Alternative for hypertriglyceridemia
1.2.3.3. AE/SE: Hepatoxicity at doses greater than 2.4g/ day; Flushing (Inc. PG synthesis) = Remedied by NSAIDs
1.2.4. Bile Acid Resins
1.2.4.1. Ex: Cholestyramine, Colestipol, Colesevelam
1.2.4.2. MOA: Binding of Bile acids which reduces liver cholesterol
1.2.4.3. Use: Add-on to statins; Useful as an antidote in Digoxin poisoning
1.2.4.4. AE/SE: Steatorrhea (Fatty Stool); Inc. risk of bile stone formation; May bind to drugs (Inc. Excretion of drugs) • Drugs with lowered absorption with Bile acid sequestrants: ADEK Vitamins, Warfarin, Digitalis
1.2.5. Cholesterol Transport Inhibitor
1.2.5.1. Ezetimibe
1.2.5.2. MOA: Inhibits NPC1-like 1 receptor; Inhibits intestinal absorption of cholesterol
1.2.5.3. Use: Add-on and synergistic with statins further lowering LDL
1.2.6. Recombinant molecules (-trapibs)
1.2.6.1. Ex: Anacetrapib, Dalcetrapib, Torcetrapib
1.2.6.2. Still on Clinical trials
1.2.7. PCSK9 inhibitor
1.2.7.1. Alirocumab
1.2.7.2. Evolocumab
1.2.8. Citrate lyase inhibitor
1.2.8.1. Bempedoic acid
2. AE/SE: Steatorrhea (Fatty Stool); Inc. risk of bile stone formation; May bind to drugs (Inc. Excretion of drugs)
3. Respiratory Disorders
3.1. Common and allergic colds
3.1.1. Drugs for Common Colds
3.1.1.1. Common Colds - viral infection
3.1.1.1.1. Top 3 causes of Viral Colds • Adenovirus • Coronavirus • Rhinovirus
3.1.2. Allergic colds
3.1.2.1. Treatment: Antihistamines (Chlorpheniramine, Brompheniramine, Diphenhydramine) and Nasal Decongestants (Phenylephrine)
3.2. Cough (w/mucus and dry cough)
3.2.1. Mucus regulators (Mucoregulators)
3.2.1.1. Ambroxol (Mucosolvan), Bromhexine, Carbocisteine (Solmux)
3.2.1.1.1. MOA: Inc. Water content of mucus and decreases viscosity of mucus
3.2.2. Mucolytic
3.2.2.1. Ex: N-acetylcysteine/NAC (Fluimucil)
3.2.2.1.1. MOA: Break disulfide bonds between mucus molecules
3.2.3. Expectorant
3.2.3.1. Ex: Guiafenasin (Mucinex) - Glyceryl guiacolate
3.2.3.1.1. MOA: Inc. Water portion of the mucus by stimulating the bronchial glands
3.2.3.1.2. Use: Management of chronic bronchitis (Excessive mucus production causing frequent cough)
3.2.4. Antitussives/Cough Suppressants
3.2.4.1. Centrally acting
3.2.4.1.1. Narcotics: Codeine, Noscapine, Papaverine
3.2.4.2. Peripherally Acting
3.2.4.2.1. Butamirate citrate (Sinecod)
3.2.4.3. Uses: - For harmful cough (TB patients); - For useless cough (Dry cough); - For excessive cough (Not used with productive cough)
3.3. Bronchospastic Disorders (Asthma and COPD)
3.3.1. Two Types: Bronchial Asthma and Chronic Obstructive Pulmonary Disease (COPD)
3.3.2. Classification based on effect: 1. Relievers (Acute attacks or exacerbation) 2. Controllers (Prevention & Maintenance)
3.3.3. Classification based on MOA 1. Bronchodilators 2. Mast cell stabilizer 3. Anti-inflammatory
3.3.3.1. Bronchodilators
3.3.3.1.1. Bronchodilator : CAMP Bronchoconstrictor: Acetylcholine, Adenosine
3.3.3.2. Mast Cell Stabilizer
3.3.3.2.1. Cromolyn sodium, Necrodomil
3.3.3.3. Anti-inflammatory drugs
3.3.3.3.1. LEUKOTRIENE MODIFIERS
3.3.3.3.2. Glucocorticoids