medical record form
by أريام العنزي
1. Provisional diagnosis
1.1. A provisional diagnosis is an initial diagnosis based on the patient's symptoms and clinical exam, pending further tests for confirmation.
2. Administrative forms
2.1. It’s used for administrative and legal documents, such as personal data, communication, and therapy bills.
2.1.1. Front sheet or identification and summary sheet
2.1.1.1. It includes identification, diagnosis, codes, doctor’s signature, and admission/discharge data.
2.1.1.2. It includes the patient's initial admission as an inpatient or outpatient.
2.1.1.3. Contents
2.1.1.3.1. The top section of a front sheet
2.1.1.3.2. The bottom section of a front shee
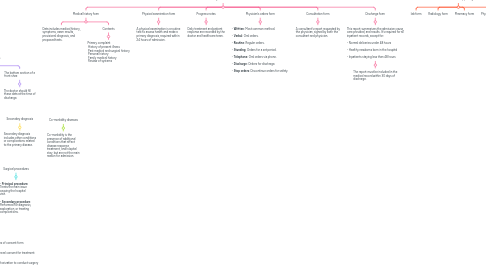
3. Physician forms
3.1. Medical history form
3.1.1. Data includes medical history, symptoms, exam results, provisional diagnosis, and proposed tests.
3.1.2. Contents
3.1.2.1. Primary complaint History of present illness Past medical and surgical history Personal history Family medical history Review of systems
3.2. Physical examination form
3.2.1. A physical examination is a routine test to assess health and make a primary diagnosis, required within 24 hours of admission.
3.3. Progress notes
3.3.1. Daily treatment and patient response are recorded by the doctor and healthcare team.
3.4. Physician’s orders form
3.4.1. - **Written**: Most common method. - **Verbal**: Oral orders. - **Routine**: Regular orders. - **Standing**: Orders for a set period. - **Telephone**: Oral orders via phone. - **Discharge**: Orders for discharge. - **Stop orders**: Discontinue orders for safety.
3.5. Consultation form
3.5.1. A consultant's report requested by the physician, signed by both the consultant and physician.
3.6. Discharge form
3.6.1. This report summarizes the admission cause, care provided, and results. It's required for all inpatient records, except for: - Normal deliveries under 48 hours - Healthy newborns born in the hospital - Inpatients staying less than 48 hours
3.6.1.1. The report must be included in the medical record within 30 days of discharge.
4. Medical Technical Supporting forms
4.1. lab form
4.2. Radiology form
4.3. Pharmacy form
4.4. Physiotherapy form
5. Final diagnosis
5.1. The final diagnosis is the main cause of the patient's current condition, determined after testing and study.
6. Secondary diagnosis
6.1. Secondary diagnosis includes other conditions or complications related to the primary disease.
7. Co-morbidity diseases
7.1. Co-morbidity is the presence of additional conditions that affect disease response, treatment, and hospital stay, but are not the main reason for admission.
8. Complications1
8.1. Complications are health issues that arise during hospital admission, affecting disease response, such as bleeding, infections, or surgical inflammation.
9. Surgical procedures
9.1. - **Principal procedure**: Treats the main issue causing the hospital visit. - **Secondary procedure**: Performed for diagnosis, exploration, or treating complications.
10. Nurses form
10.1. Nurse’s notes
10.2. Vital signs forms
10.3. medications report
11. Surgical operations forms
11.1. Operative reports
11.2. Anesthesia report
12. The outpatient clinic
12.1. Outpatient clinics treat minor conditions like infections, injuries, and common illnesses.
12.2. In some countries, nurses see general outpatients, who typically don't need an appointment.
12.3. Patient-held health records help reduce the daily filing burden for outpatient records.
13. Problems associted outpatient Medical Record
13.1. The patient doesn't bring the health record to outpatient visits.
13.2. The health record has been lost.
13.3. The health record has been tampered with.
14. Deposition:
14.1. Used to summarize the case at discharge, with terms like cured, improved, or expired (died).
15. أريام خالد مكيمن العنزي
16. Examples of consent form
16.1. General consent for treatment
16.2. Authorization to conduct surgery
16.3. Authorization to release information from the MR
16.4. Discharge against medical advice consent and refuse the treatment
16.5. Agreement to receive multiple treatments

