
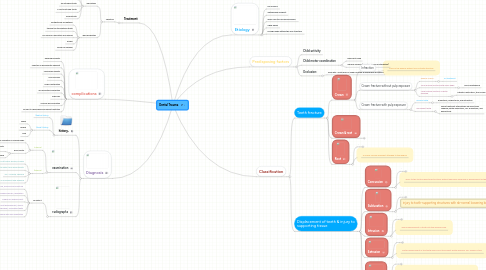
1. Diagnosis
1.1. history,
1.1.1. Medical history
1.1.2. Dental History
1.1.2.1. When
1.1.2.2. Where
1.1.2.3. How
1.2. examination
1.2.1. Intraoral
1.2.1.1. Soft tissue: laceration or foreign body
1.2.1.2. Each Tooth:
1.2.1.2.1. Fracture ,dislocation , or mobility. Palpation and percussion.
1.2.1.2.2. Vitality testing : not routine & not reliable
1.2.2. Extraoral
1.2.2.1. Soft tissue: wound, bruises
1.2.2.2. Facial skeleton : palpated to detect any discontinuity
1.2.2.3. TMJ: clicking, swelling
1.2.2.4. Mandibular movement: pain stiffness, limitation in movement and opening
1.3. radiographs
1.3.1. To detect:
1.3.1.1. Root fracture, alveolar bone fracture
1.3.1.2. Radiolucencies, resorption
1.3.1.3. Degree of displacement
1.3.1.4. Extent of root development, size of the pulp chamber, unerupted teeth
1.3.1.5. Baseline data documentation
2. complications
2.1. Reversible pulpits
2.2. Infection in periodontal ligament
2.3. Irreversible pulpitis
2.4. Pulp necrosis
2.5. Pulpal obliteration
2.6. Inf lammatory resorption
2.7. Ankylosis
2.8. Coronal discolouration
2.9. Injuries to developing permanent dentition
3. Treatment
3.1. Splinting
3.1.1. Indications
3.1.1.1. Anavulsed tooth
3.1.1.2. A displaced tooth
3.1.1.3. An extruded tooth
3.1.1.4. A root fractured tooth
3.1.1.5. mobiletooth
3.1.2. Ideal properties
3.1.2.1. Aesthetically acceptable
3.1.2.2. tabilize the traumatized teeth
3.1.2.3. No need for laboratory procedures
3.1.2.4. simple
3.1.2.5. Cause no damage
4. Etiology
4.1. Fall injuries
4.2. Automobile accident
4.3. Injury due to convulsive seizure
4.4. Child abuse
4.5. Foreign body hitting the oral structure
5. Predisposing factors
5.1. Child activity
5.2. Child motor coordination
5.2.1. learning to walk
5.2.2. medical problem ( mental , physical retardation)
5.3. Occlusion:
5.3.1. open bite : protrusion of upper centrals & insufficient lip closure
6. Classification
6.1. Teeth fracture
6.1.1. Crown
6.1.1.1. Infraction
6.1.1.1.1. crack of the enamel without loss of tooth structure.
6.1.1.2. Crown fracture without pulp exposure
6.1.1.2.1. Enamel cracks :
6.1.1.2.2. Small Enamel fracture with sharp edge
6.1.1.2.3. Large enamel fracture & dentin exposed
6.1.1.3. Crown fracture with pulp exposure
6.1.1.3.1. Primary teeth
6.1.1.3.2. Permanent teeth
6.1.2. Crown & root
6.1.2.1. Treatment
6.1.2.1.1. Permanent teeth
6.1.2.1.2. Primary teeth
6.1.3. Root
6.1.3.1. .
6.1.3.1.1. Treatment
6.1.3.2. A mobile coronal fragment attached to the gingiva.
6.2. Displacement of teeth & injury to supporting tissue
6.2.1. Concussion
6.2.1.1. .
6.2.1.1.1. Treatment
6.2.1.2. injury to the tooth-supporting structures without abnormal loosening or displacement of the tooth.
6.2.2. Subluxation
6.2.2.1. .
6.2.2.1.1. Treatment
6.2.2.2. injury to tooth-supporting structures with ab-normal loosening but without tooth displacement.
6.2.3. Intrusion
6.2.3.1. .
6.2.3.1.1. Treatment
6.2.3.2. Apical displacement of tooth into the alveolar bone.
6.2.4. Extrusion
6.2.4.1. .
6.2.4.1.1. Treatment
6.2.4.2. partial displacement of the tooth axially from the socket; partial avulsion. PDL usually is torn.
6.2.5. Avulsion
6.2.5.1. .
6.2.5.1.1. Treatment
6.2.5.2. complete displacement of tooth out of socket. PDL is severed and fracture of the alveolus may occur.