
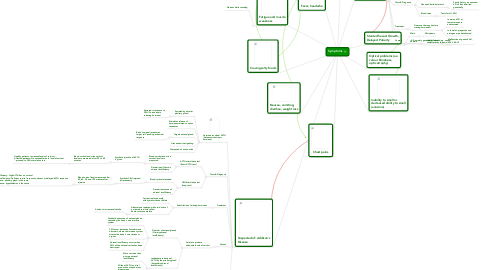
1. Fatigue and muscle weakness
1.1. Worsens while standing
2. Darkened skin colour (hyperpigmentation)
2.1. Tanned skin in places not exposed to sun
2.2. Old scars darken
2.3. Darkening common in creases of hands
3. Fever, headache
4. Nausea, vomiting, diarrhea, weight loss
5. Craving salty foods
6. Chest pains
7. Suspected of: Addison's Disease
7.1. Hormone involved: ACTH (Adrenocorticotropic hormone)
7.1.1. Secreted by anterior pituitary gland
7.1.1.1. Secreted in response to CRH (Corticotropin releasing hormone)
7.1.2. Stimulates release of hormones related to stress responses
7.1.3. Targets adrenal gland
7.1.3.1. Binds to signal receptor on target cell, invoking a chemical response
7.1.4. Uses endocrine signaling
7.1.5. Composed of amino acids
7.2. Tests & Diagnosis
7.2.1. ACTH stimulation test (Short ACTH test)
7.2.1.1. Blood cortisol and urine cortisol levels are measured
7.2.1.1.1. Synthetic injection of ACTH is given
7.2.1.2. Determines if there is adrenal insufficiency
7.2.2. CRH Stimulation test (Long test)
7.2.2.1. Blood cortisol measured
7.2.2.1.1. Synthetic CRH injected intravenously
7.2.2.2. Determines cause of adrenal insufficiency
7.3. Treatment
7.3.1. Substitution of missing hormones
7.3.1.1. Cortisol replaced orally with hydrocortisone tablets
7.3.1.2. Aldosterone replaced with oral doses of a mineralocorticoid called fludrocortisone acetate
7.3.1.2.1. Advise to increase salt intake
7.4. Causes
7.4.1. Failure to produce adequate levels of cortisol
7.4.1.1. Disorder of adrenal glands (Primary adrenal insufficiency)
7.4.1.1.1. Gradual destruction of adrenal glands, caused by the body's own immune system
7.4.1.1.2. 70% occur because of autoimmune disorders, where the immune system attacks the body's own tissues or organs
7.4.1.1.3. Adrenal insufficiency occurs when 90% of the adrenal cortex has been destroyed
7.4.1.2. Inadequate secretion of ACTH by the pituitary gland (Secondary adrenal insufficiency)
7.4.1.2.1. More common than primary adrenal insufficiency
7.4.1.2.2. Without ACTH, cortisol production drops but not aldosterone
7.5. Addisonian Crisis
7.5.1. Severe case of Addison's, result of undiagnosed Addison's disease or intercurrent problem in someone who has Addison's
7.5.2. Severe symptoms
7.5.2.1. Sudden pain in legs and back
7.5.2.2. Severe vomiting and diarrhea resulting in dehydration
7.5.2.3. Severe lethargy
7.5.2.4. Confusion, slurred speech
7.5.2.5. Hypoglycemia
7.5.2.6. Convulsions
7.5.3. Treat with intravenous injections of hydrocortisone, saline and dextrose (sugar), treatment is immediate
7.5.3.1. When severity has decreased, treat with oral medication
8. Inability to smell or decreased ability to smell (anosmia)
9. Stunted Sexual Growth, Delayed Puberty
9.1. Male
9.1.1. Micropenis
9.2. Female
9.2.1. delayed secondary sexual characteristics (breasts)
10. Optical problems (ex. colour blindness, optic atrophy)
11. Suspected of: Kallmann Syndrome
11.1. Hormone involved: LH (Lutenizing hormone)
11.1.1. Secreted by anterior pituitary gland
11.1.1.1. Release from pituitary gland controlled by GnRH (Gonadotropin releasing hormone)
11.1.1.1.1. New node
11.1.2. Targets gonads (testes, ovaries)
11.1.2.1. In females, acts on ovarian follicle, inducing ovulation and maintaining corpus luteum
11.1.2.2. In males, acts on Leydig cells of testes to produce testosterone
11.1.3. Glycoprotein
11.2. Tests & Diagnosis
11.2.1. Smell test to assess degree of anosmia
11.2.1.1. Absent or exceptionally weak sense of smell is an indicator of KS
11.2.2. Gene and heriditary tests
11.2.2.1. Family history is examined. KS is often inherited genetically
11.2.3. Blood tests
11.2.3.1. Tests for LH, FSH
11.3. Treatment
11.3.1. Hormone therapy (restore missing hormones)
11.3.1.1. In males, hCG or testosterone are adminstered
11.3.1.2. In females, progestins and estrogen are administered
11.4. Causes
11.4.1. KS is mainly genetically linked
11.4.1.1. Malfunction of genes KAL1, KAL2, KAL3